Clinical Practice Guideline for Optima Prone
Risk Factors and Development of Pressure Injuries
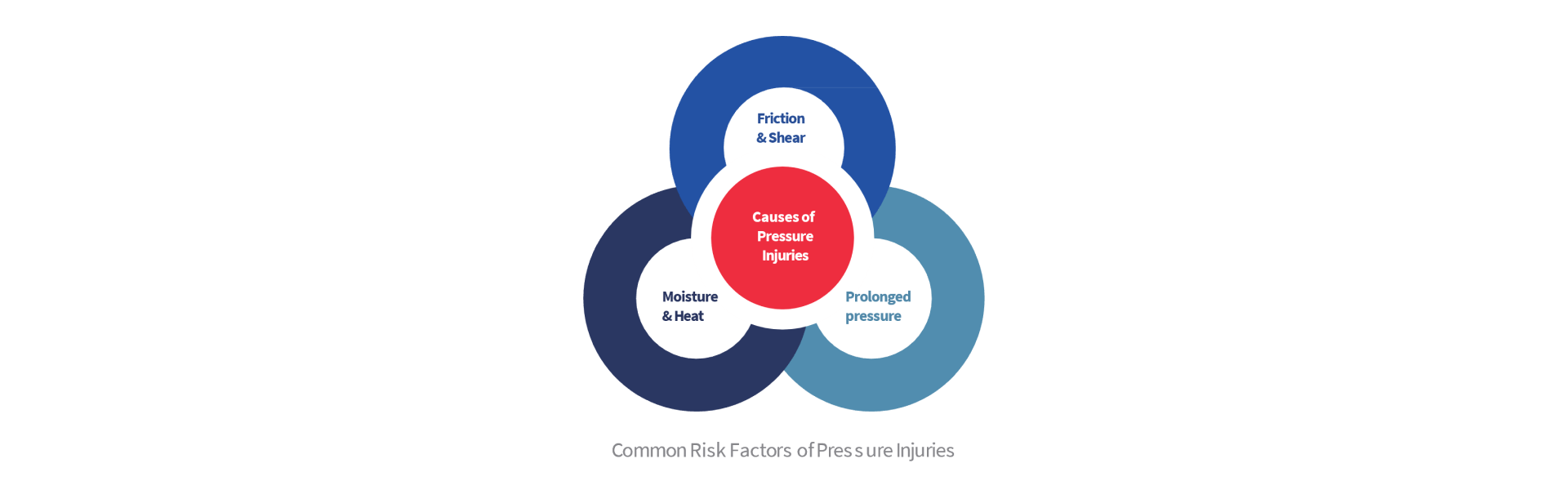
Pressure Injuries commonly occur as a result of tissue being exposed to prolonged pressure or pressure associated with friction & shear, or the weaker tissue caused by moisture.1
Pressure injuries are categorized into 6 stages2 : Stage I with a non-blanchable erythema of intact skin; Stage II with a partial-thickness skin loss with exposed dermis; Stage III with a full-thickness skin loss; Stage IV with a full-thickness skin and tissue loss; Unstageable pressure injury is defined as obscured full thickness skin and tissue loss; And last, Deep tissue pressure injury is the persistent non-blanchable deep red, maroon or purple discoloration of the skin.
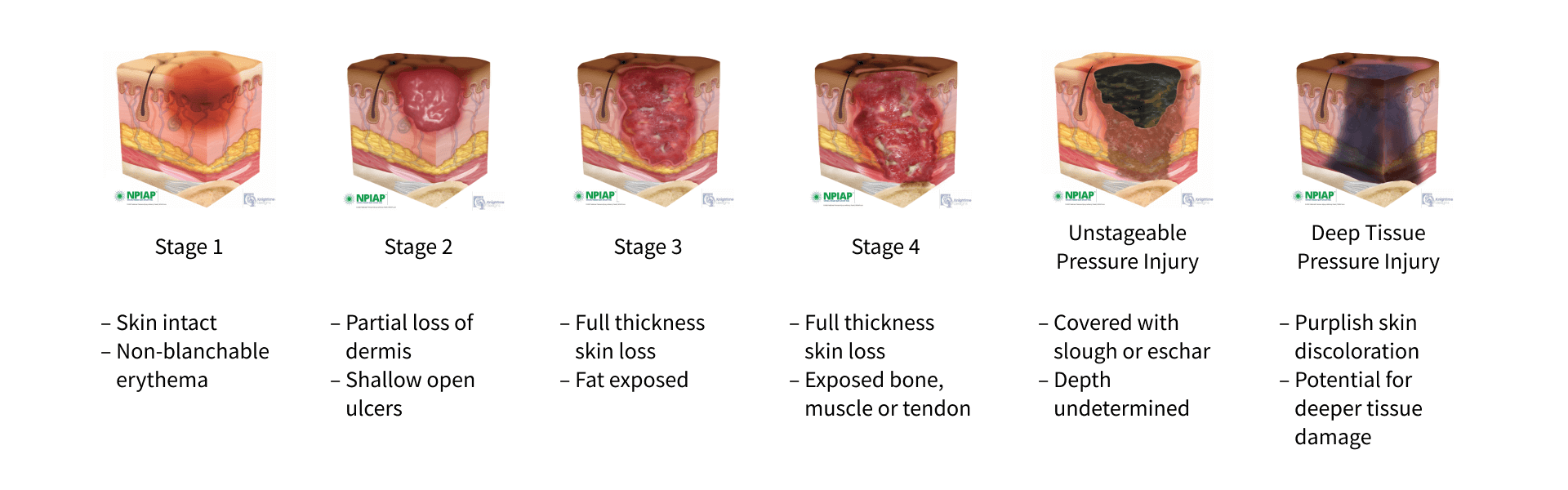
Images used with permission from https://npiap.com/page/PressureInjuryStages
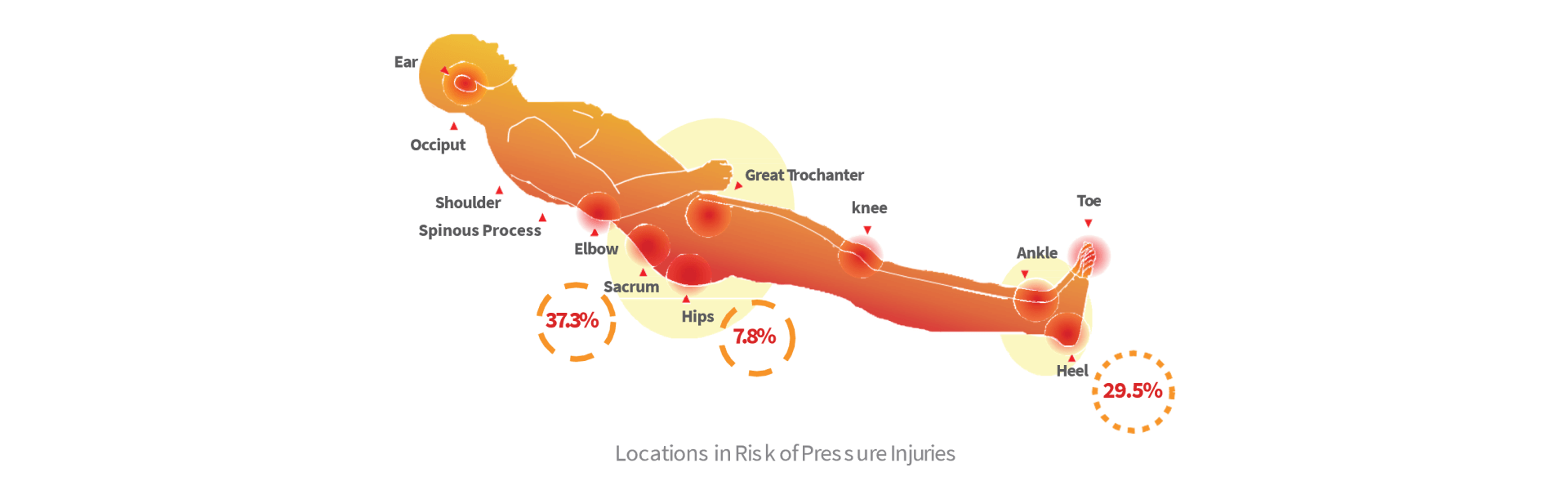
They may be superficial injuries affecting the epidermis and dermis or they can extend into the subcutaneous tissues and involve muscle, tendon and bone. Pressure injuries typically occur over bony prominences with the lower trunk (sacrum, coccyx, trochanter and ischial tuberosity) and heels being the two most common anatomical locations.3,4
Localized areas of tissues that have prolonged pressure cause the occlusion of blood flow, preventing the supply of nutrients and oxygen to the tissue, resulting in ischaemia and re-perfusion injury, leading to cell obliteration and eventually tissue death.5
From the information of the mechanism of pressure injuries above, additional risk factors that have been correlated with are age of 70 years and older, current smoking history, dry skin, low body mass index, impaired mobility, altered mental status (i.e., confusion), diabetes mellitus, peripheral vascular disease, urinary and fecal incontinence, malnutrition, physical restraints, malignancy, history of pressure injuries, and human race.
Pressure injuries can develop within 2 to 6 hours. Therefore, the key to preventing pressure injuries is to accurately identify at-risk individuals quickly, so that preventive measures may be implemented.6 A major method of redistributing pressure is the use of support surfaces. Many researches had been conducted on the effectiveness of the use of support surfaces in reducing the incidence of pressure injuries. The concept of pressure redistribution has been embraced by the NPIAP.
"Support surfaces are: "Specialized devices for pressure redistribution"7
"Support surfaces are specialized devices for pressure redistribution designed for management of tissue loads, microclimate, and/or other therapeutic functions (i.e., any mattress, integrated bed system, mattress replacement, overlay, or seat cushion, or seat cushion overlay)".7 In this context, pressure refers to the distribution of force on the individual’s body surface that is in contact with the device.
"Evaluate the individual’s comfort when using an alternating pressure air mattress or overlay. Powered alternating pressure air mattresses and overlays can be noisy and generate heat or motion that may be uncomfortable".8
Optima Prone
Pressure Mapping
By investigating the pressure mapping of Optima Prone, we can use the software to analyze the Pressure Area Index (PAI) and Pressure Redistribution Index (PRI) of different modes to see the performance of product, when threshold of interface pressure gets stricter, you can find out that Optima Prone can still offer good performance for prevention of pressure injuries.
Equipment Used: The XSENSOR X3 Display Medical Mattress System
Software Used: Xsensor X3 medical V6
Method : Each test is conducted over a 30-minute period during which the average, peak and minimum pressures are recorded.
Pressure Area Index (PAI): Pressure Area Index (PAI) is a method used to measure the interface pressure of the surface. The PAI is calculated as the proportion of sensors that register interface pressure values.9
Pressure Redistribution Index (PRI): Pressure Redistribution Index (PRI) is a method to assess the ability of a dynamic support surface to sustain interface pressures below a chosen set of thresholds. The PRI is calculated as the ratio of the time during which the dynamic support surface interface pressure trace spends below the threshold and the total time of one inflation/deflation cycle.10
Product Therapy Modes and Performance
Sitting Position: PAI & pressure mapping test of Optima Prone in
the sitting position for 30 minutes. User Height: 175 cm, User Weight: 110 Kg, BMI: 35.9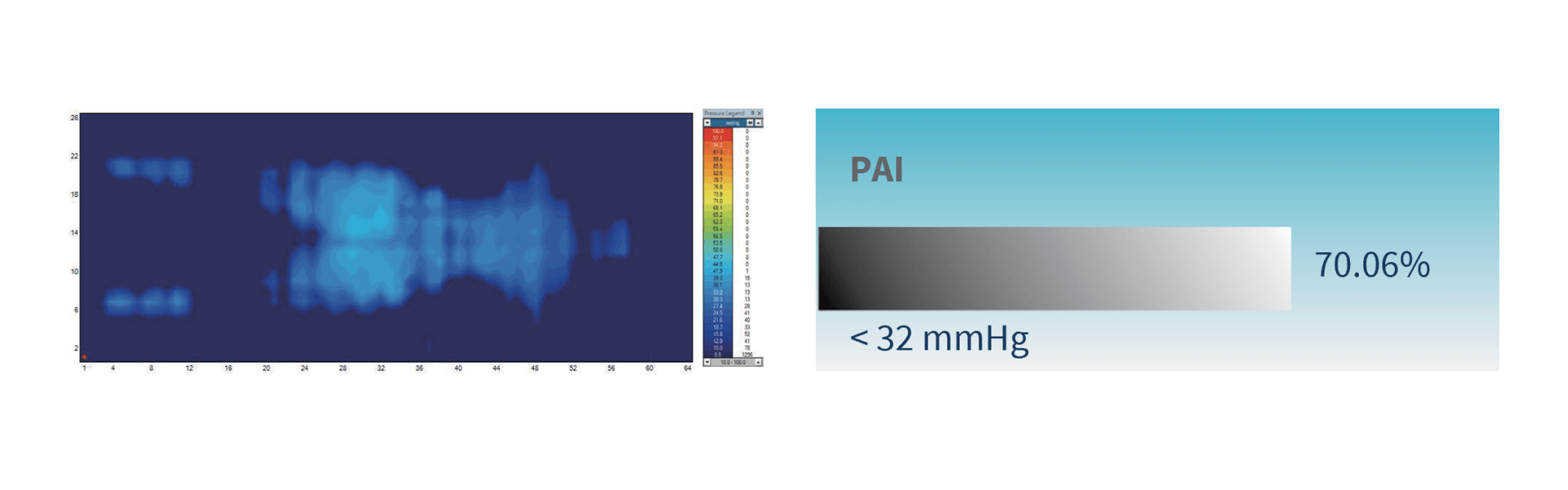
Optima Prone (when used in Continuous Low Pressure mode) reaches a maximum of 28.8 mmHg and a minimum of 26.4
mmHg, and the 100% of interface pressures during its 30-minute cycle are all below 32 mmHg.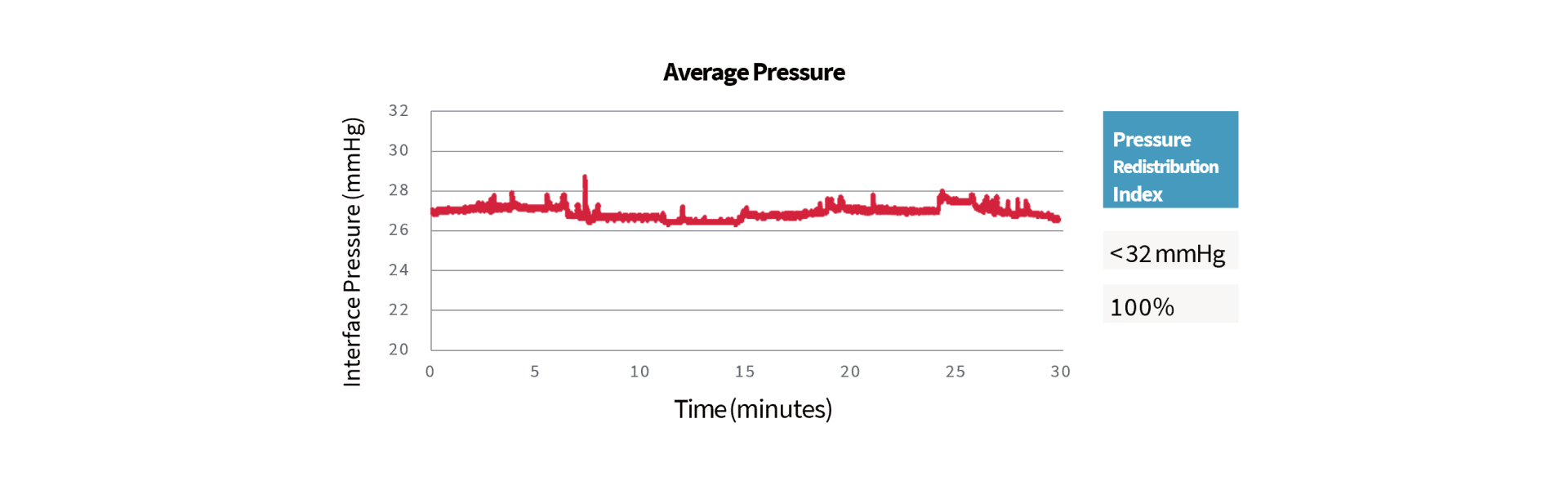
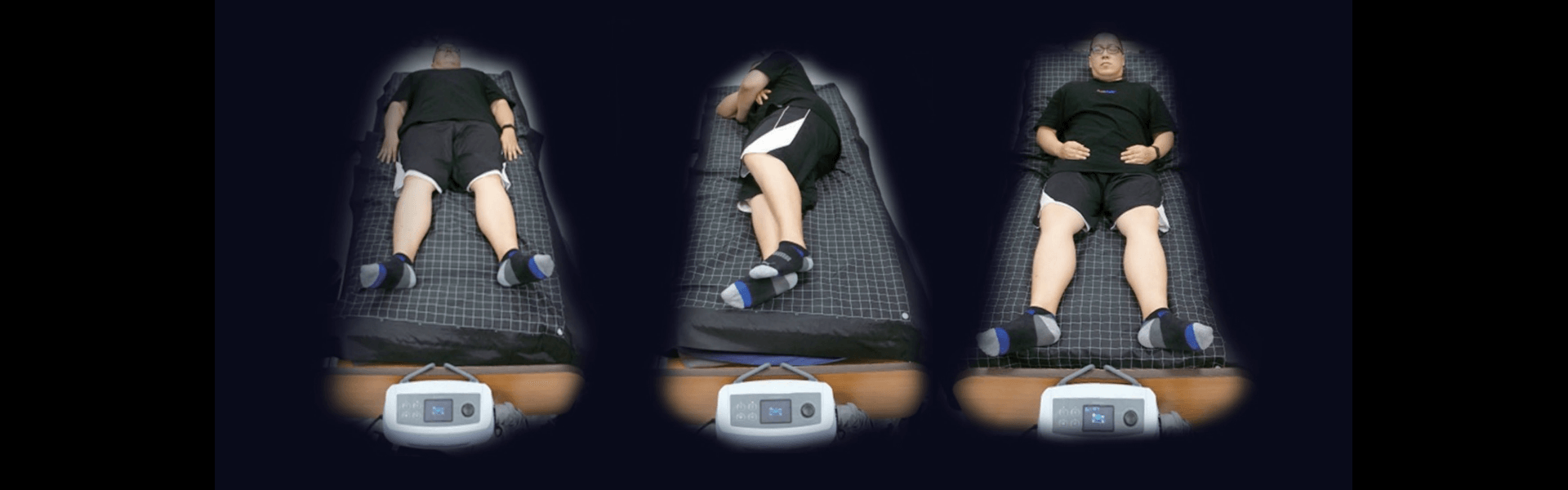
Alternating Mode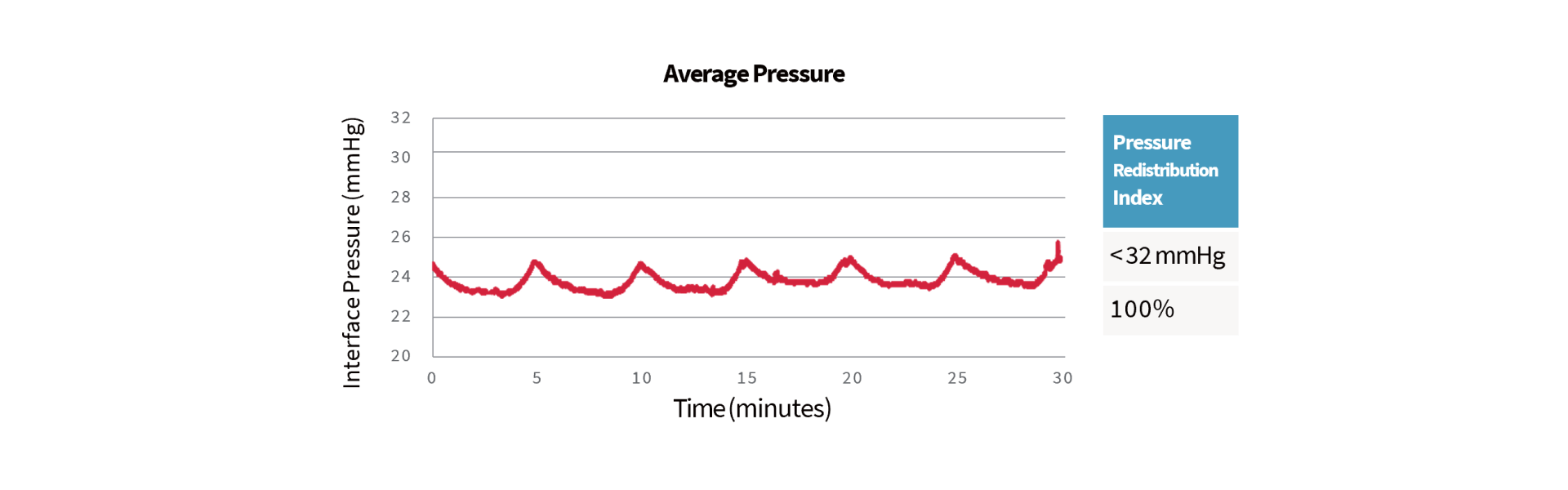
From the
pressure mapping images you can easily observe the alternating situation in the supine position: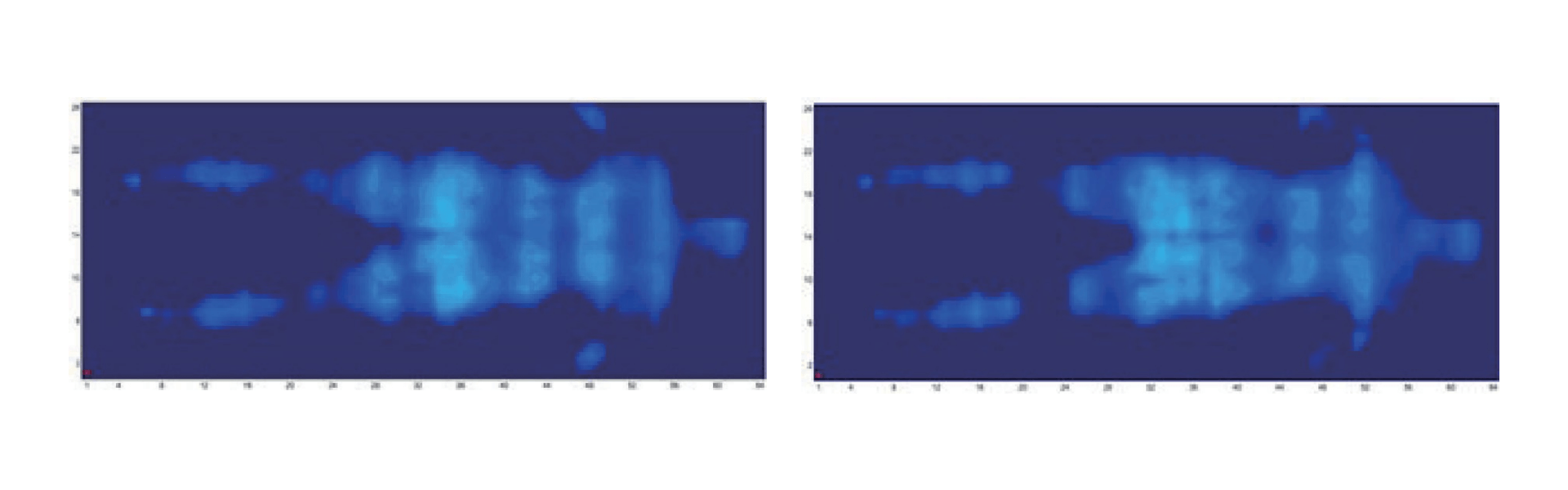
Lateral Position: PAI & pressure mapping test of Optima Prone in
the lateral position for 30 minutes. User Height: 175 cm, User Weight: 110 Kg, BMI: 35.9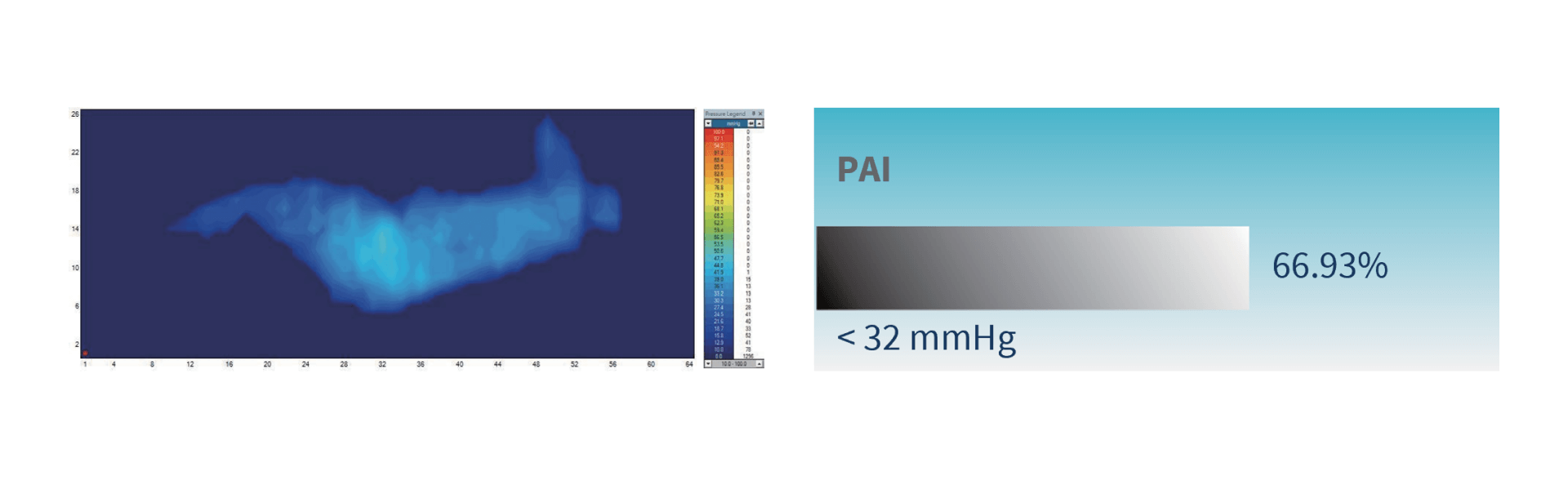 Optima Prone
(when used in alternating mode) reaches a maximum of 29.5 mmHg and a minimum of 27.3 mmHg, and the 100% of
interface pressures during its 30-minute cycle are all below 32 mmHg.
Optima Prone
(when used in alternating mode) reaches a maximum of 29.5 mmHg and a minimum of 27.3 mmHg, and the 100% of
interface pressures during its 30-minute cycle are all below 32 mmHg.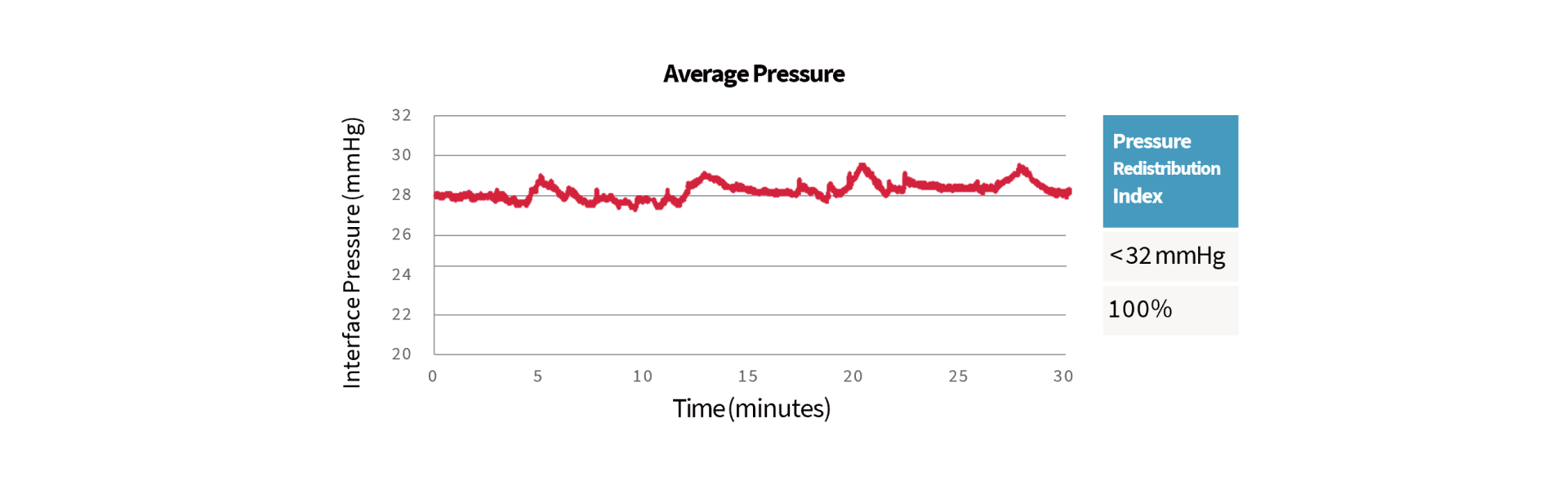
From the
pressure mapping images you can easily observe the alternating situation in the lateral position: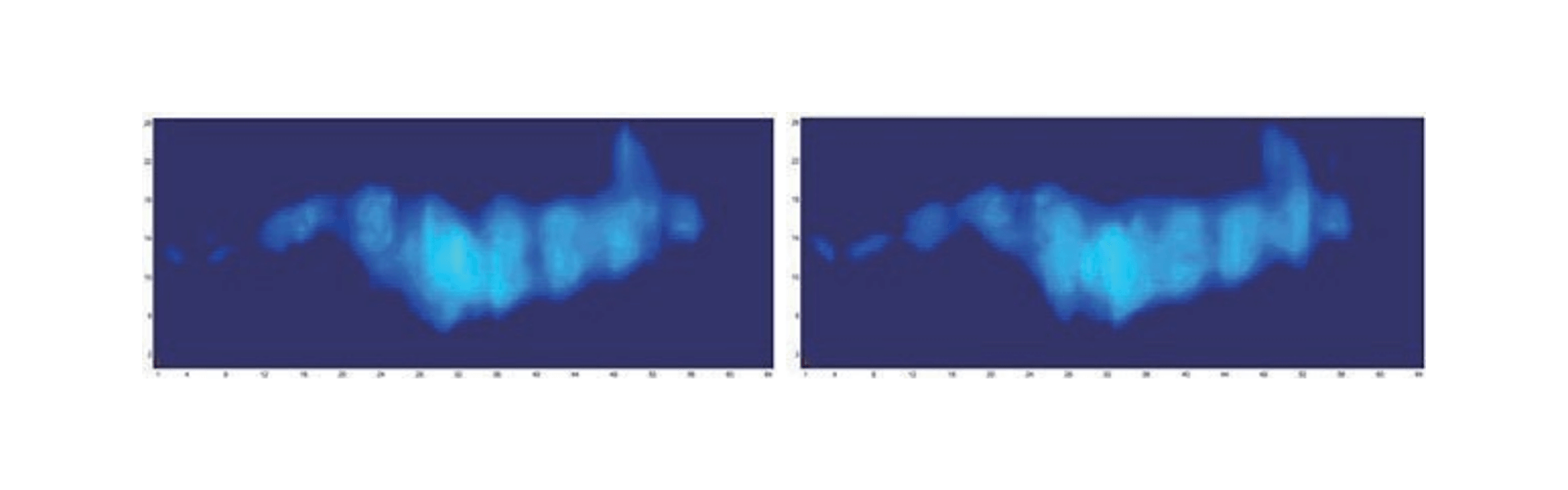
Sitting Position: PAI & pressure mapping test of Pro-care Optima
in the sitting position for 30 minutes. User Height: 175 cm, User Weight: 110 Kg, BMI: 35.9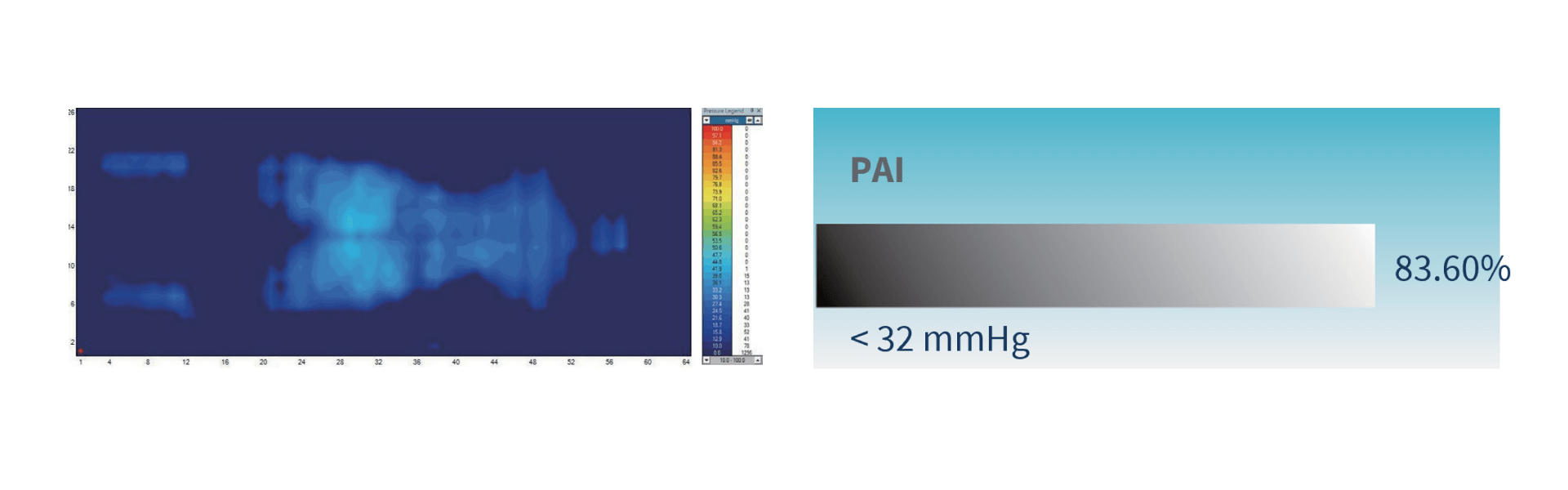 Optima Prone
(when used in alternating mode) reaches a maximum of 29.3 mmHg and a minimum of 24.4 mmHg, and the 100% of
interface pressures during its 30-minute cycle are all below 32 mmHg.
Optima Prone
(when used in alternating mode) reaches a maximum of 29.3 mmHg and a minimum of 24.4 mmHg, and the 100% of
interface pressures during its 30-minute cycle are all below 32 mmHg.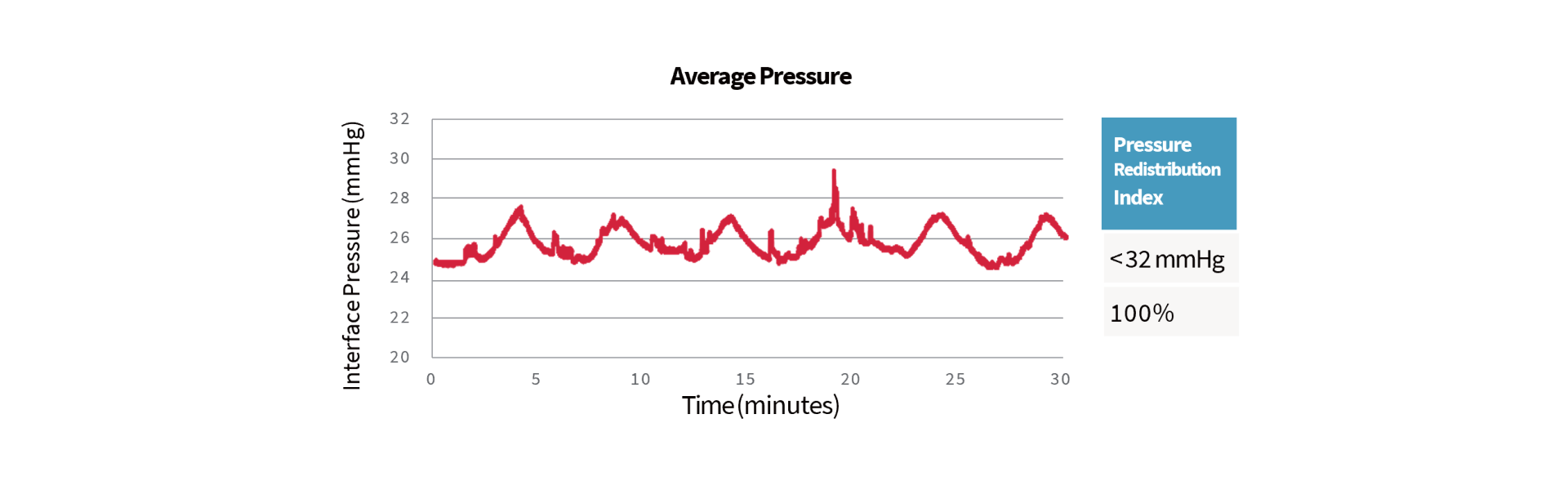
From the
pressure mapping images you can easily observe the alternating situation in the sitting position: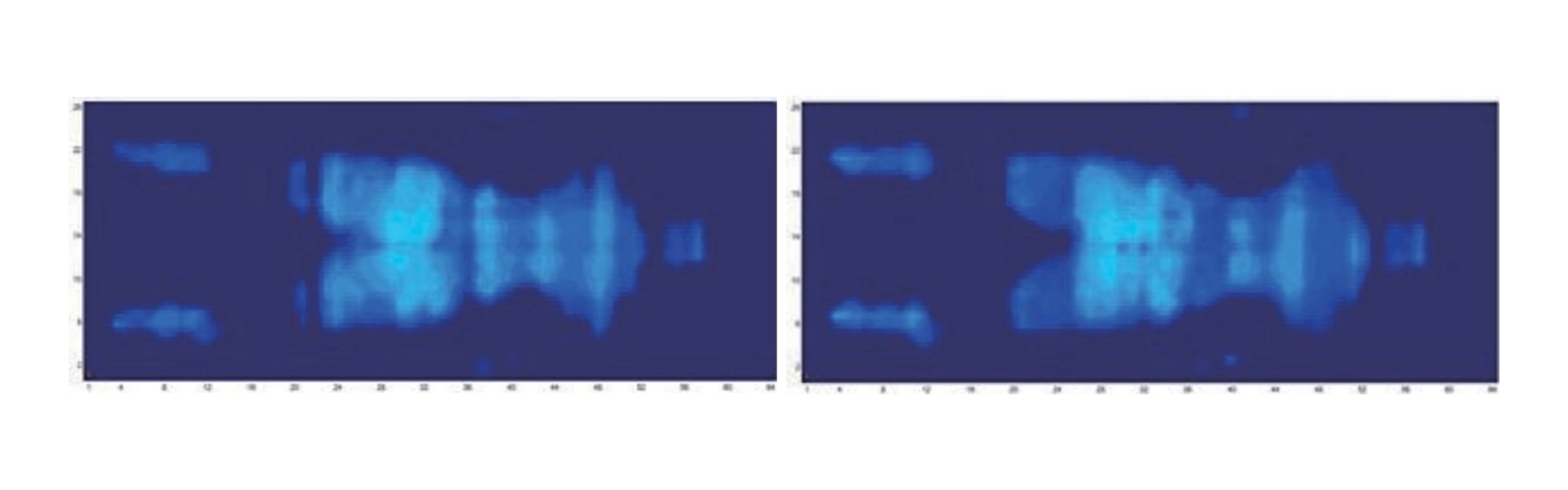
"Assess the relative benefits of using an alternating pressure air mattress or
overlay for individuals at risk of pressure injuries"13
Optima Prone (when used in alternating mode) reaches a maximum of 25.9 mmHg and a minimum of 23.1 mmHg, and the
100% of interface pressures during its 30-minute cycle are all below 32 mmHg.
Multi-zone Air Pressure
"Pressure redistribution is achieved by either increasing the body surface
area that comes in contact with the support surface through immersion and envelopment (to reduce
concentrations of weight over bony prominences)."14
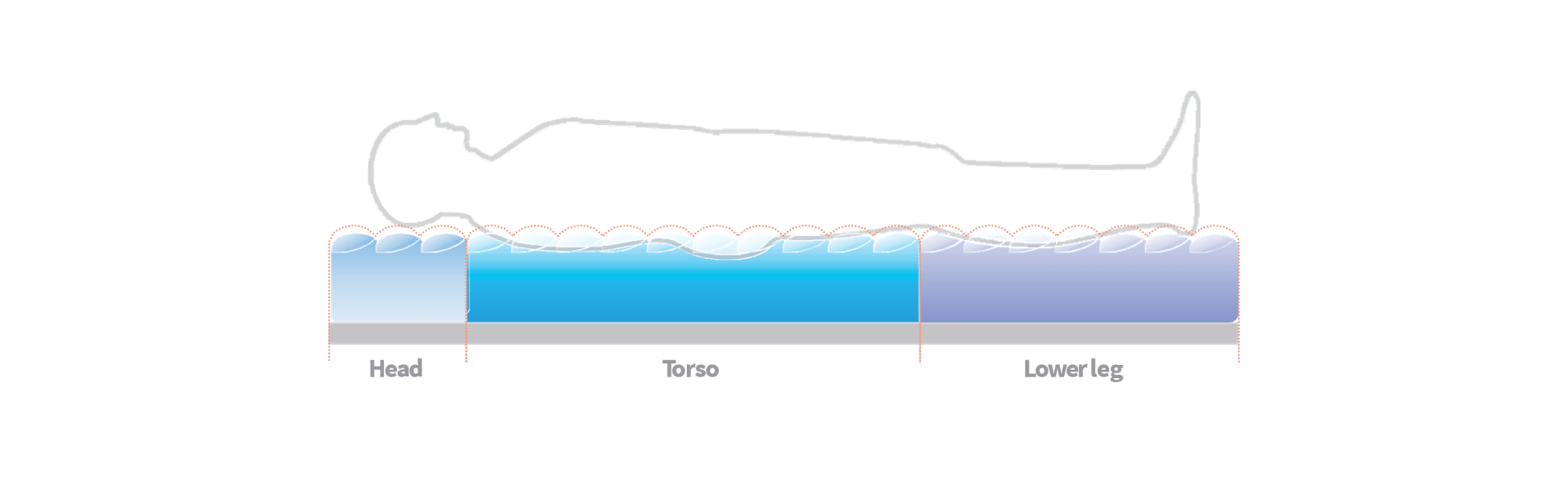
In consideration of the body segment mass and anatomical structures, the mattress of Optima Prone is divided into
three zones: Head, torso and lower leg.
Torso accounts for more than 40% of the body weight and areas such as scapula, sacrum, and hip are susceptible to pressure injuries.15 For instance, sacrum is known as the most common anatomical sites for pressure injuries16 due to its thinner soft tissue17, 18 and is located at the end of the spinal column, which is exposed to higher pressure.18
Providing with different inner pressure in each zone, Multi-zone Air Pressure demonstrates significant pressure redistribution to fit different patient contours with stability and comfort by better immersion and envelopment.
An in-house
single-blinded test was done to evaluate the comfort level that Multi-zone Air Pressure offers to the
participants.
73% (11 out of 15 users) would prefer the optimal comfort Multi-zone Air Pressure provides. In addition, there
was a 20% increase in satisfaction percentage showing the comfort level was relatively higher in mattress with
Multi-zone Air Pressure.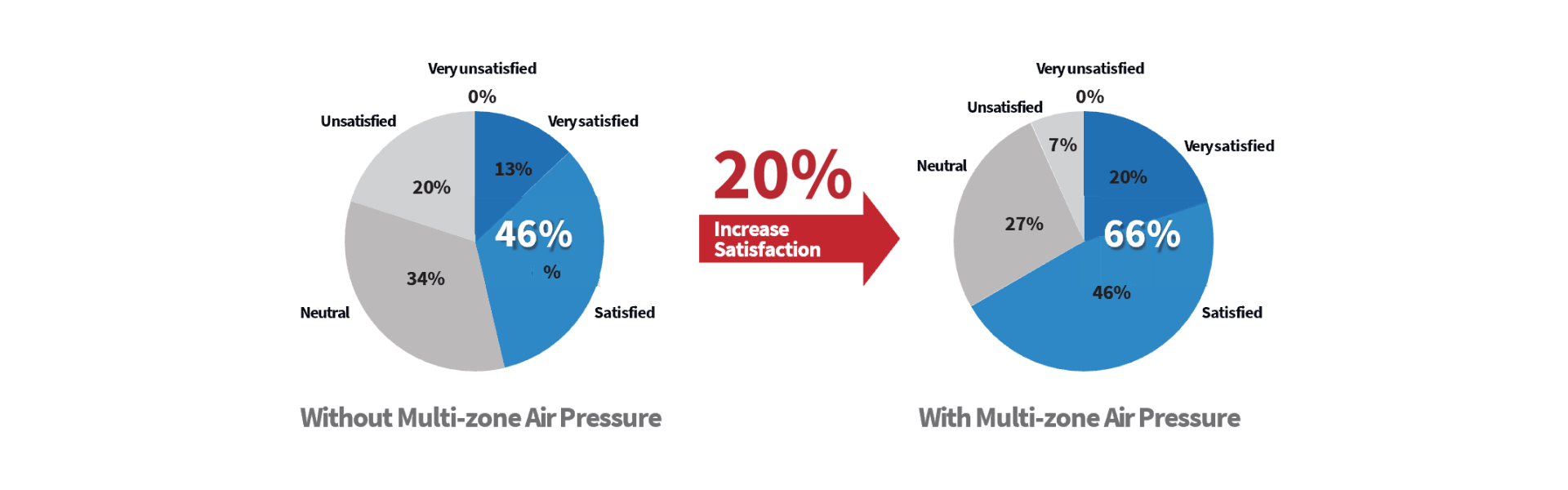
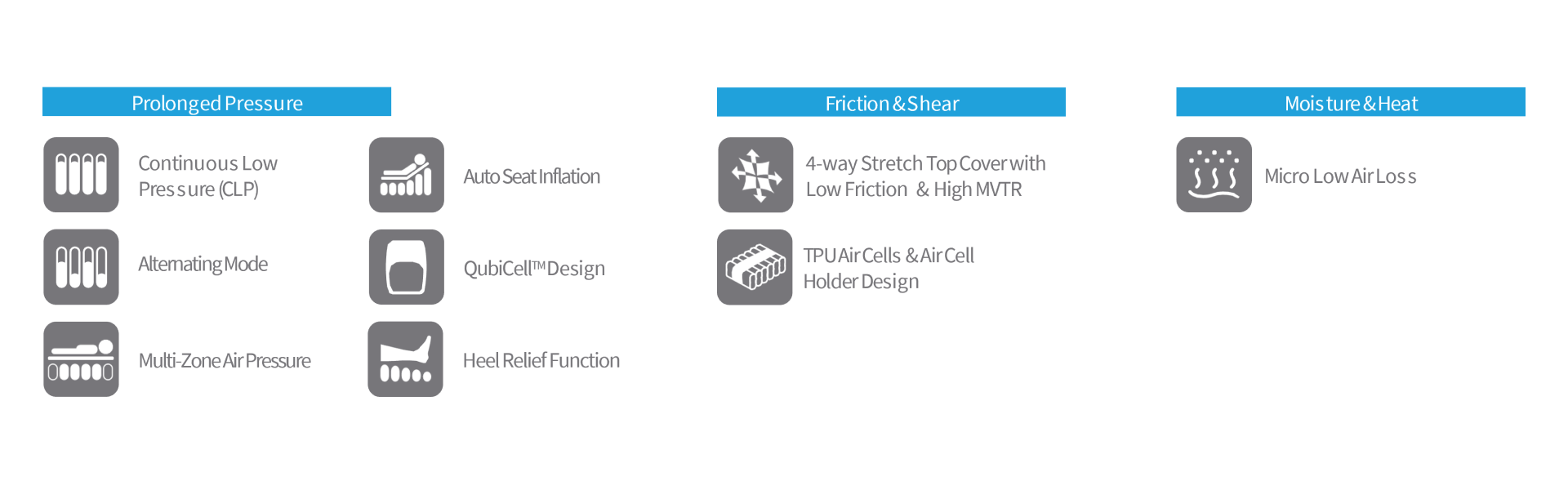
Auto Seat Inflation
"For individuals with a pressure injury, consider changing to a specialty support
surface when the individual: ‘Bottoms out’ on the current support surface."19
To avoid the situation of bottoming out, Optima Prone offers an Auto Seat Inflation function, which
automatically inflates when the head section has been raised by ≥ 30°, and provides extra support in
sacral area during sitting position. The pressure in the whole mattress increases when the patient is in a
fowler’s position for a steady support.
Optima Prone is also equipped with 6 Cell-in-Cell air cells at sacrum area, by which provide excellent support
for the patient in sitting-up position or when exiting and entering the mattress.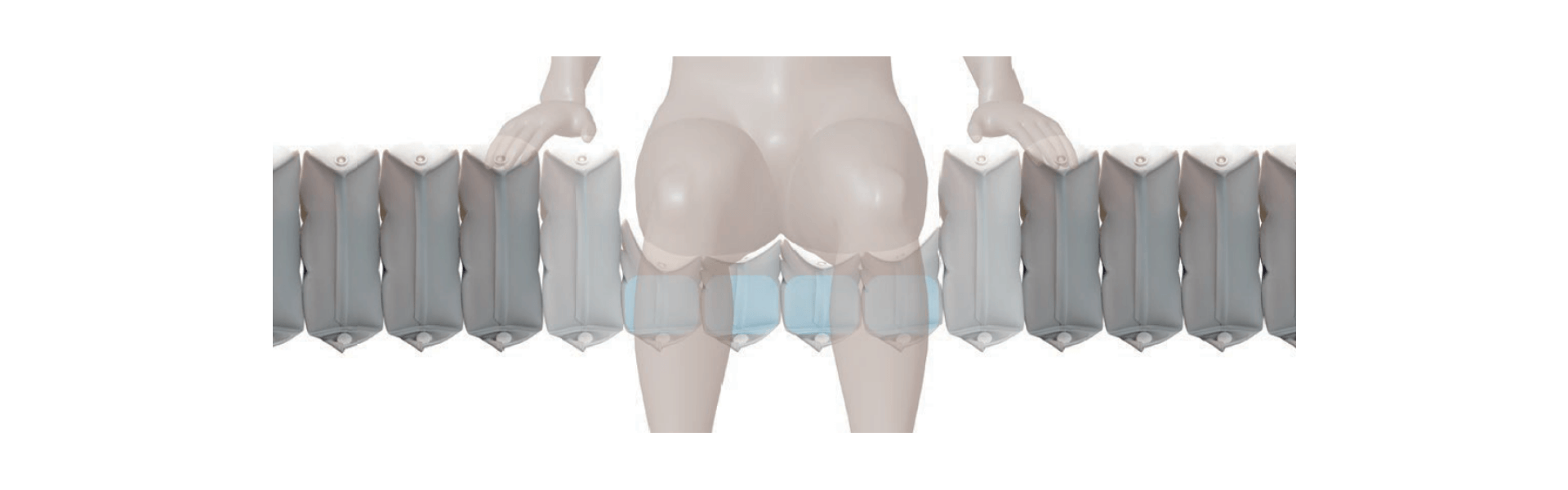
CPR Operation
CPR knob is located at the patient’s left-hand side of the mattress near the head section area. Whenever a CPR
operation is needed, quickly turn the CPR knob to release air from the mattress. The CPR deflation time is
within 15 seconds. The quick connector on the pump unit can be disconnected for an even faster deflation
process.
QubiCellTM
"Evaluate the safety of alternating pressure air mattresses and overlays
when in use. Some individuals may experience difficulty getting into and out of the bed when an
alternating pressure air mattress or overlay is in use."20
Optima Prone consists of 21 rectangular cells, providing a larger contact area and thus lower interface pressure in supine position.
Thanks to its solenoid valve technology, it can enable more stable & comfortable alternating cycles - it inflates odd air cells before deflating even air cells (and vice-versa) during the alternating process by turning the valves on and off sequentially to provide an effective therapy in high comfort for the patient.
TPU Air Cells & Air Cell Holder Design
Thermoplastic polyurethanes (TPU) air cells used for Optima Prone mattress are highly resistant to hydrolysis,
soft, less friction and even less noisy when patient is moving their body on the mattress, its material
chose and the design of the air cell holders are in aids with reducing friction & shear forces for the
patient lying in different postures.
LCD Monitor
Optima Prone pump is equipped with a control knob without grooves (which has been designed for helping prevention
of cross infection) and a LCD screen with an intuitive graphic design to save time and effort for operation and
troubleshoot, reducing the chance of misuse.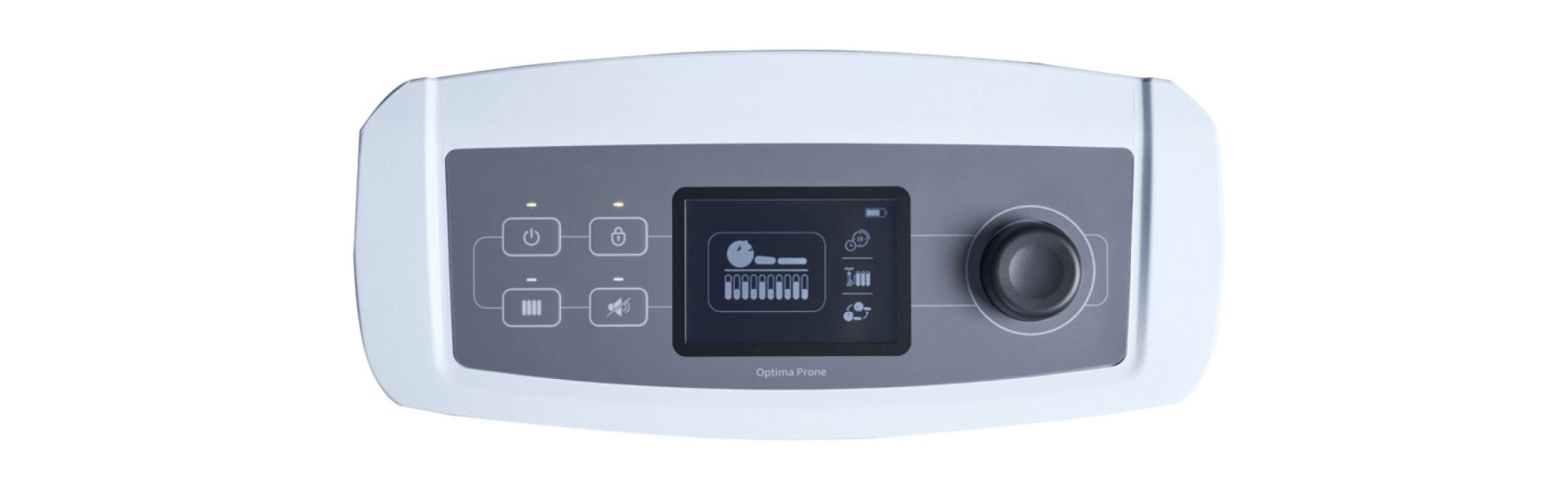
Heel Relief Function
"The heel is one of the two most common anatomical sites for pressure injuries. In a European survey on pressure injury prevalence, almost 80% of all Category/Stage IV pressure injuries were found at the sacrum and heels."21
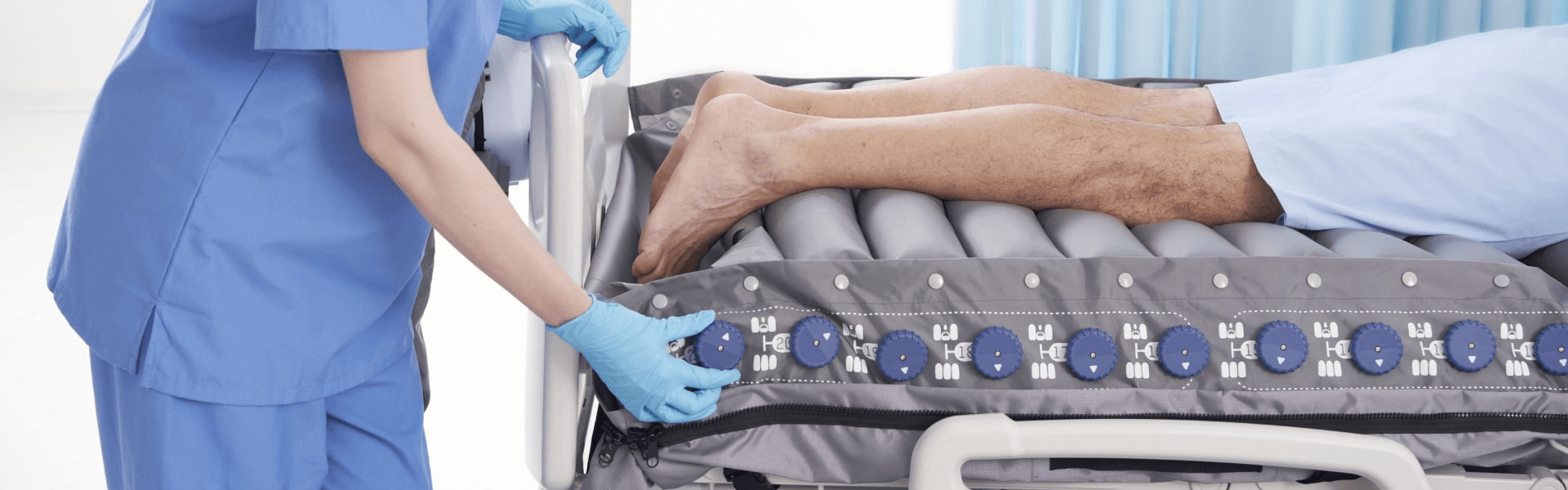
Heel Relief Function is a simple and easy way to prevent and assist in treating heel pressure injuries by
eliminating interface pressure from heels as if they are suspended in air. The heel is typically reported as the
second most common sites for pressure injury development.21
One of the
five knobs in the lower leg section can be deflated according to the patient’s heel location to achieve
zero pressure.
Top Cover
"Consider using textiles with low friction coeAcients for individuals with or at risk of pressure injuries."22
Optima Prone alternating pressure redistribution system is provided with a standard cover (sanitary cover sheet) with high-performance technical material which covers them completely and is biocompatible, with low friction (μ = 0.21 (static), μ = 0.17 (dynamic)) & shear forces, water resistant and highly vapor permeable.
The Moisture vapor transmission rate (MVTR) is 2315 g/24hrs/m2 according to ASTM E96 Procedure
BW.
Microclimate Management
"An increasing body of evidence suggests that the microclimate between skin and
the supporting surface plays a role in the development of pressure injuries."23
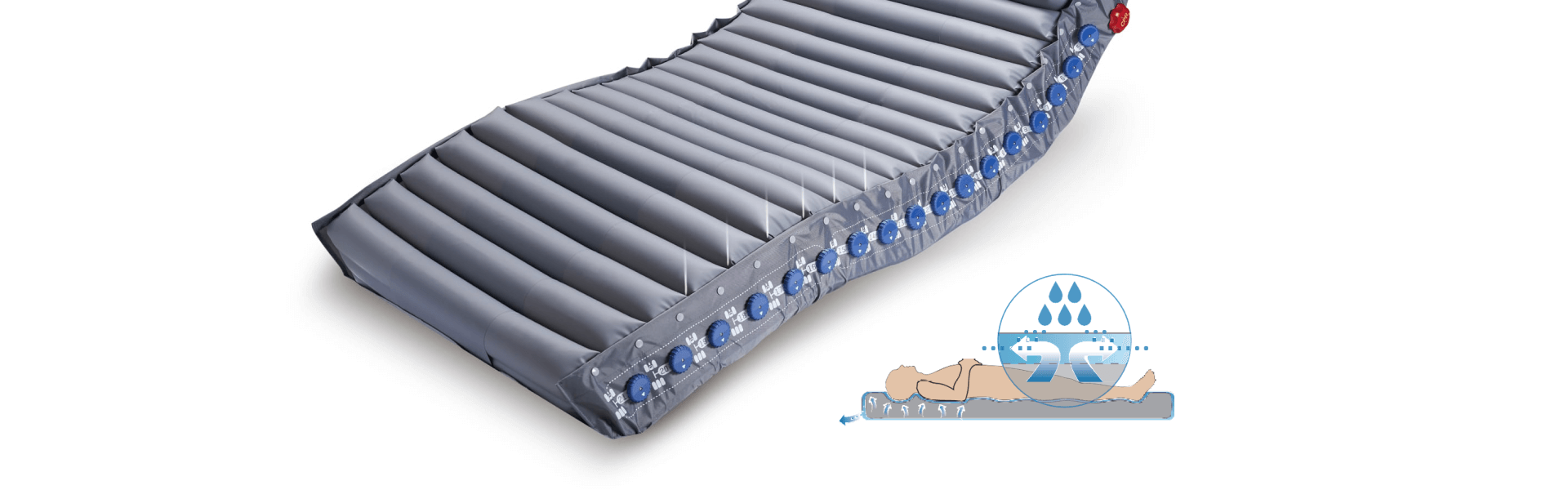
As for the
microclimate control, Optima Prone offers micro low air loss function, which provides good ventilation and
reduces the accumulation of heat and moisture.
Transport Mode &
Power Failure
"Contingency plans for power failure should be in place."24
The Optima Prone with optional battery pack can offer a non-stop dynamic pressure relief for up to 6 hours in
addition to the 24 hours the standard mattress system can remain inflated during power failure or patient
transfer.
Design of Saving Time
The air cells with quick release detachable base on Optima Prone can be easily removed from mattress during decontamination which can save up to 80% of time compared to regular mattress systems.
Optima Prone is also equipped with a cable management feature which can reduce tripping hazards for a safer
healthcare environment.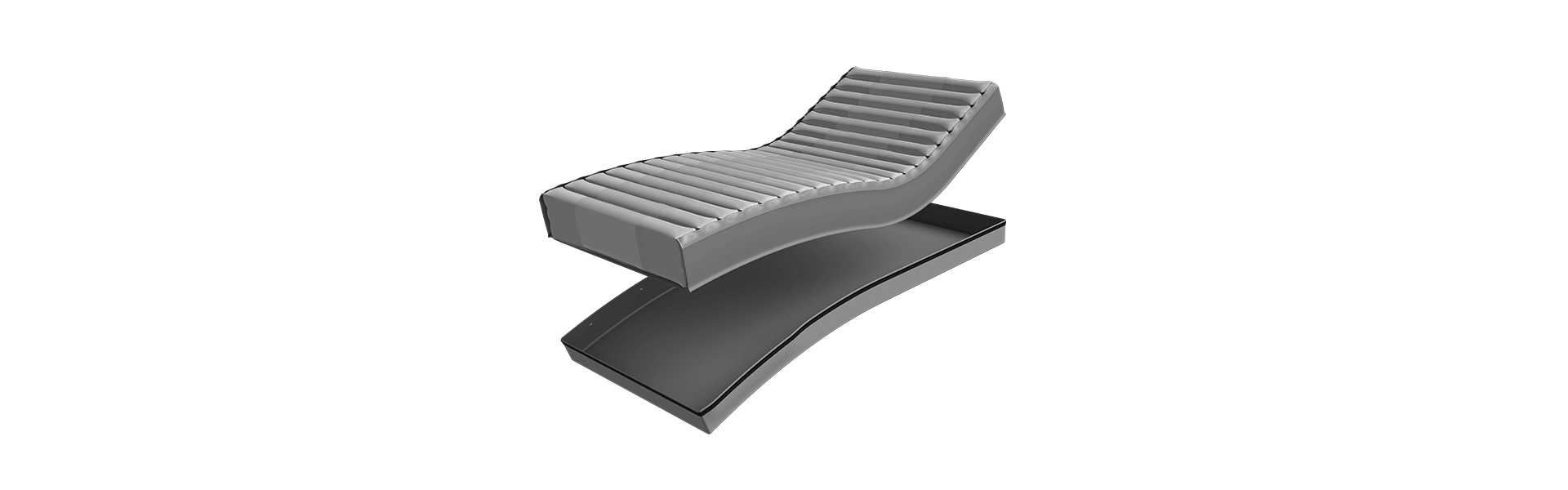
Initial Inflation
Once the pump recognizes the mattress size through the quick connector, it will begin to inflate mattress which takes less than 30 minutes to complete the initial inflation.

Continuous Low Pressure (CLP)
"Consider using a reactive air mattress or overlay for individuals at risk for
developing pressure injuries"11
Once the pump recognizes the mattress size through the quick connector, it will begin to inflate mattress which takes less than 30 minutes to complete the initial inflation. Reactive air mattresses redistribute pressure by deforming in response to an individual’s weight on the surface.12 Optima Prone offers a Continuous Low Pressure mode, which provides a stable surface with a pressure lower than the corresponding level when in the alternating mode. Also, this therapy mode is for the patients who are not fond of vibrations or alternating sensations.
Supine Position: PAI & pressure mapping test of Optima Prone in the supine position for 30 minutes. User Height: 175 cm, User Weight: 110 Kg, BMI: 35.9
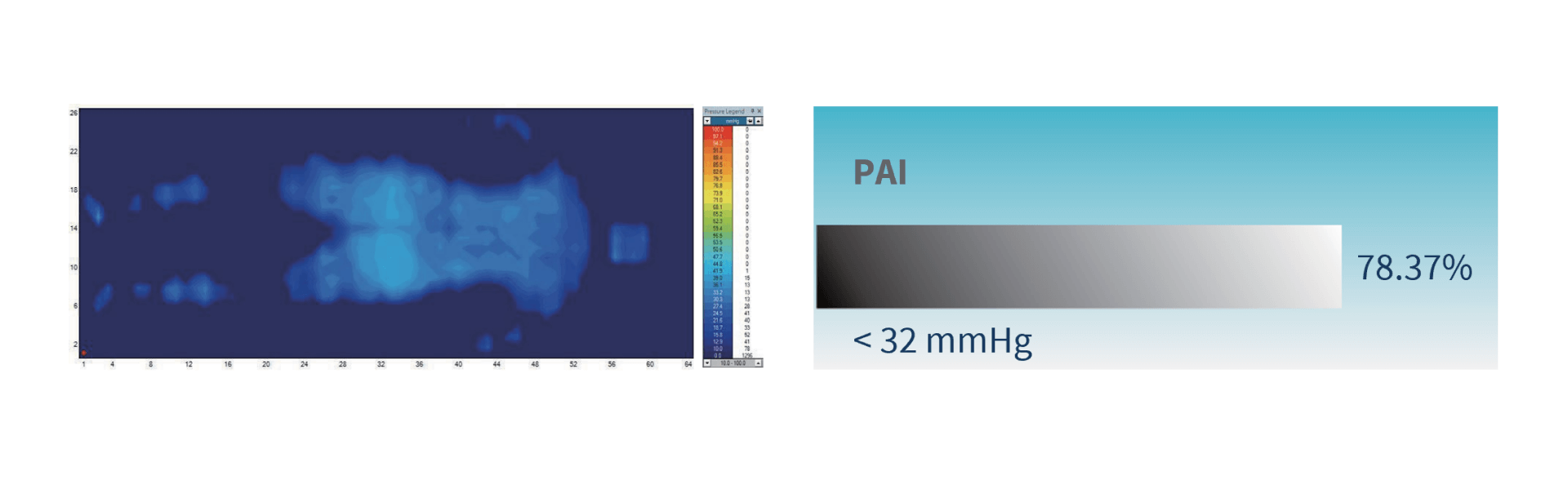
Optima Prone (when used in Continuous Low Pressure mode) reaches a maximum of 27.6 mmHg and a minimum of 24.8
mmHg, and the 100% of interface pressures during its 30-minute cycle are all below 32 mmHg. 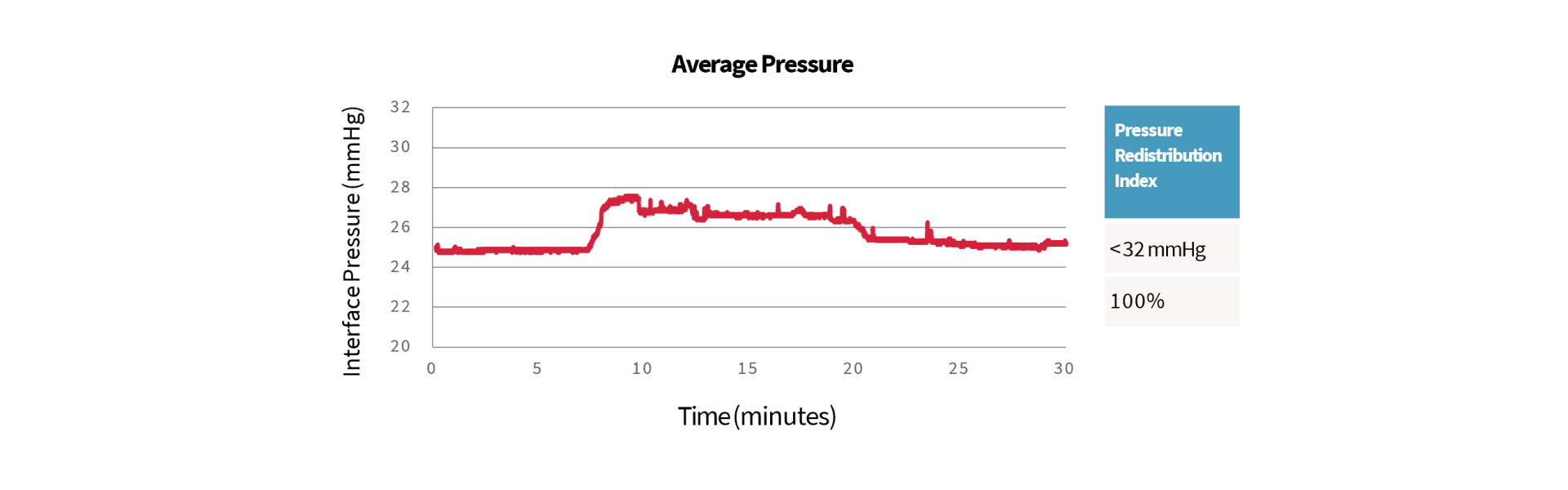
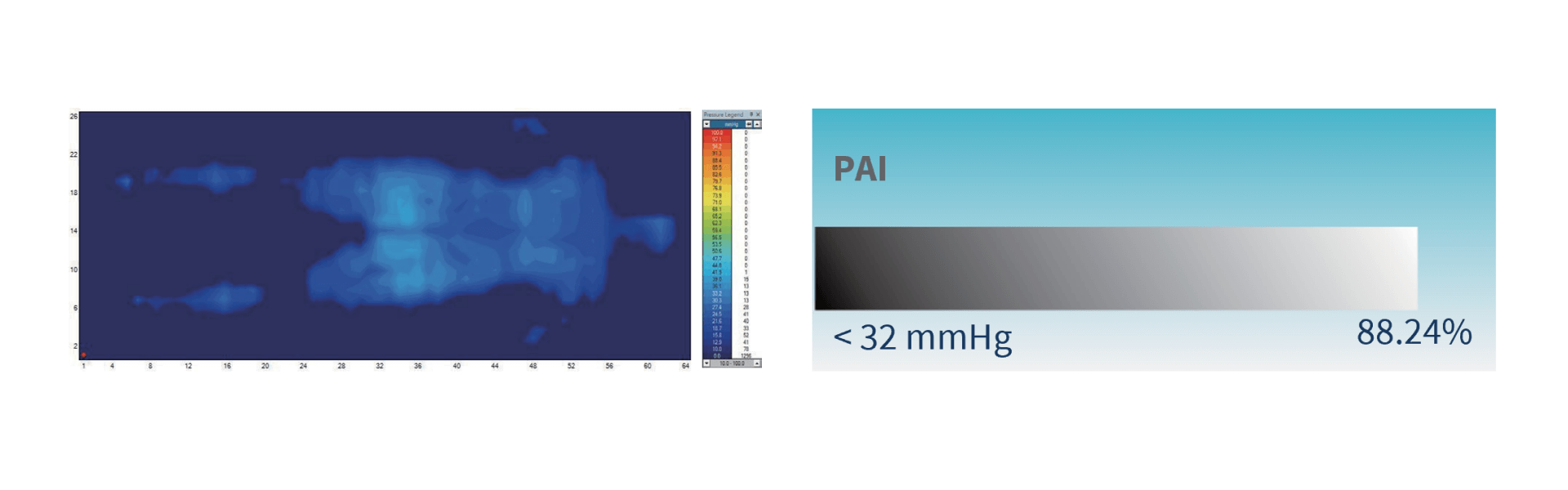
Lateral Position: PAI & pressure mapping test of Optima Prone in
the lateral position for 30 minutes. User Height: 175 cm, User Weight: 110 Kg , BMI: 35.9
Optima Prone (when used in Continuous Low Pressure mode) reaches a maximum of 29.1 mmHg and a minimum of 28.0
mmHg, and the 100% of interface pressures during its 30-minute cycle are all below 32 mmHg.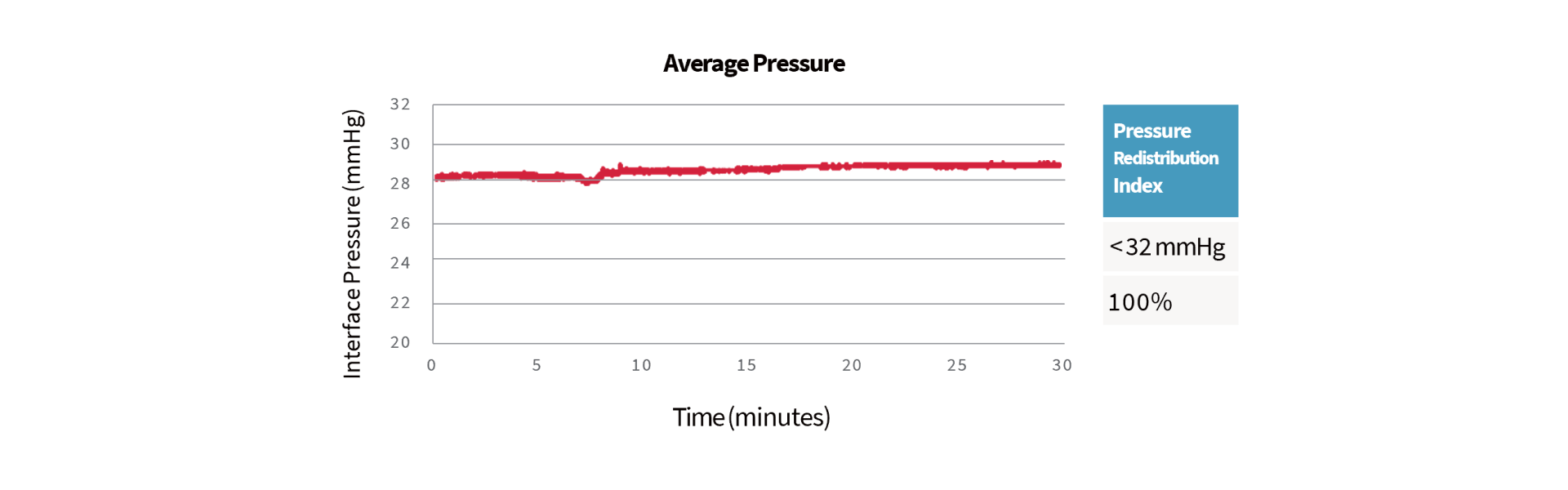
Optima Prone offers an alternating mode, which continuously and sequentially inflate and deflate air cells (1-in-2 alternating) to avoid long term pressurization of tissue, and also provides four kinds of operating cycle time (10, 15, 20, 25 min).
Supine Position: PAI & pressure mapping test of Optima Prone in the supine position for 30 minutes. User Height: 175 cm, User Weight: 110 Kg, BMI: 35.9
Frequently Asked Questions (FAQ)
References
1. Karen Hertz. 2018. Fragility Fracture Nursing. USA: Springer
2. NPIAP Pressure Injury Stages (https://cdn.ymaws.com/npiap.com/resource/resmgr/online_store/npiap_pressure_injury_stages.pdf)
3. Zhaoyu Li, Frances Lin, Lukman Thalib, Wendy Chaboyer. 2020. Global prevalence and incidence of pressure injuries in hospitalized adult patients: a systematic review and meta-analysis. Journal of Nursing Studies.
4. Gawlitta D, Li W, Oomens CW, Baaijens FP, Bader DL, Bouten CV. 2007 The relative contributions of compression and hypoxia to development of muscle tissue damage: an in vitro study. Annals of Biomedical Engineering. 35(2), 273-84.
The references listed below by page number, refer to direct statements appearing in the full version of the European Pressure Ulcer Advisory Panel, National Pressure Injury Advisory Panel and Pan Pacific Pressure Injury Alliance. Prevention and Treatment of Pressure Ulcers/Injuries: Clinical Practice Guideline. The International Guideline, Emily Haesler (Ed.).EPUAP/NPIAP/PPIA:2019.
5. Section 5: Skin and Tissue Assessment. Page 74
6. International review. Pressure ulcer prevention: pressure, shear, friction and microclimate in context. A consensus document. London: Wounds International, 2010.
7. Section 10: Support Surfaces. Page 155
8. Section 10: Support Surfaces. Page 166
9. Kenney L, Rithalia SVS. 1999. Mattress & bed resource file: assessment of support surfaces. J Wound Care (Suppl); Part 2: 1-8.
10. Twiste M, Rithalia S. 2008. Measurement system for the evaluation of alternating pressure redistribution mattresses using pressure relief index and tissue perfusion– a preliminary study. Wound Practice and Research. Volume 16
11. Section 10: Support Surfaces: Recommendation 7.5. Page 163
12. Malbrain M, Hendriks B, Wijnands P, Denie D, Jans A, Vanpellicom J, De Keulenaer B. 2010. A pilot randomised controlled trial comparing reactive air and active alternating pressure mattresses in the prevention and treatment of pressure ulcers among medical ICU patients. J Tissue Viability. 19(1), 7-15.
13. Section 10: Support Surfaces: Recommendation 7.7. Page 165
14. Section 10: Support Surfaces. Page 159
15. Robert K. Jensen. 1989. Changes in segment inertia proportions between 4 and 20 years. Journal of Biomechanics.
16. Section 9: Heel Pressure Injuries. Page 145
17. Clark M, Rowland LB, Wood HA, Crow RA. 1989. Measurement of soft tissue thickness over the sacrum of elderly hospital patients using B-mode ultrasound. J Biomed Eng.
18. Abed Elahad, J., McCarthy, M.W., Goverman, J. et al. 2018. An Overview of Sacral Decubitus Ulcer. Curr Trauma Rep.
19. Section 10: Support Surfaces: Good Practice Statement 7.9. Page 169
20. Section 10: Support Surfaces. Page 166
21. Section 9: Heel Pressure Injuries. Page 145
22. Section 6: Preventive Skin Care: Recommendation 3.4. Page 88
23. Section 2: Etiology. Page 22
24. Section 10: Support Surfaces. Page 157
